

How do you know when a patient is lying about his symptoms, condition and history? The short answer is “you don’t.” But, as this case study will demonstrate, you need to use all your senses, especially your powers of observation.
Accusing anyone of lying is serious business, but when that person is your patient, the stakes are even higher. But what do you do when a patient really is telling a lie?
How do you know when a patient is lying about his symptoms, condition and history? The short answer is “you don’t.” But, as this case study will demonstrate, you need to use all your senses, especially your powers of observation.
ADVERTISEMENT
My patient, a 33-year-old African American male, was brought from the front seat of a Greyhound bus by ambulance to the community emergency room where I was moonlighting near the end of my third year of residency.
He reported that he had a known diagnosis of an ascending aortic dissection and was traveling from his home in Miami, Florida to see a vascular surgeon in Seattle, Washington. Aortic dissection is not a common diagnosis, occurring with an incidence of 3.5 per 100,000 per year [7]. It is frequently life-threatening, and an acute presentation requires emergent and often surgical intervention. He reported that, while on the bus, he developed chest pain, feeling both like an elephant sitting on his chest, as well as a more severe, tearing pain radiating into his back that felt like his aortic dissection. He had a past medical history of Ehlers-Danlos syndrome and chronic myelogenous leukemia, currently in remission, as well as multiple previous pneumothoraces and thromboses, both deep venous and pulmonary.
He stated he had previously had an operation performed in Munich, Germany where his dissection had been “clipped,” but not permanently repaired, and also reported placement of an inferior vena cava filter. He claimed to have anaphylactic allergies to CT contrast, propofol, sulfa drugs, ketamine, and droperidol. He had poor peripheral veins and requested almost immediately that a central line be placed. He carried with him a well-worn copy of a transesophageal echocardiogram (TEE) report showing a possible intimal flap near his aortic valve. Initial vital signs showed a BP of 117/72 and HR of 110.
ADVERTISEMENT
Physical exam revealed a thin, pale male with a medial sternotomy scar, a port scar in his upper right chest, and several scars on his lateral chest consistent with previous chest tubes.
Prior to medical school, I lived in Germany while serving in the military, so I conversationally asked him why he was there (attempting to build rapport but also curious about the consistency of his responses). He told me that he had been an ROTC student at Stuttgart and periodically driven to Munich. I commented this was a long drive, and he reported it had taken him 12 hours each time (this is a two and one half hour drive). I asked him whether he spoke German and he said that he did, but was not able to answer simple questions in German. Something did not smell right. What stood out to me was how mechanically he described his complaint and history, offering a textbook description of both angina and aortic dissection. He rattled off his list of allergies as though he’d said it a hundred times. Few patients are that fluent with their medical history.
In addition, the description of his previous surgical intervention was quite circumspect — that a surgeon would intervene with an open-chested surgery without performing the definitive operation for his diagnosis would be a considerable deviation from the standard of care. But with his complicated past and the scars to prove it, I gave him the benefit of the doubt.
ADVERTISEMENT
My desire to do the right thing and care for the patient carried me forward. I was able to place an ultrasound-guided peripheral line and thereby negate his request for a central line. We administered a dose of IV esmolol and fentanyl upon his request. CT angiography is the test of choice for evaluation of aortic dissection and in the setting of a contrast allergy we will often pretreat with steroids and antihistamines.
He utterly refused this. I offered an MR angiogram of his aorta. He replied that the metal in his chest prevented him from having an MRI. As a former MRI tech well versed in contraindications, I assured him that having an MRI would pose no risk; but he continued to refuse, saying that his previous doctors had told him he could not have one. He requested instead that we obtain a TEE, which would require sedation which, due to his allergies, would have to be performed at least in part with narcotics.
At this point I had the opportunity to review our records, which were connected by our electronic medical record (EMR) with several associated hospitals. I discovered that he had presented to one such hospital in another state in 2011 with an identical complaint with the exception that he had been traveling from California to Kansas for his repair at that time. He had been admitted to that hospital and after an extensive workup they found no evidence of dissection. In fact, they noted that the week prior to his presentation there, he had been seen in more than ten different hospitals in the Las Vegas area.
Turning to my technological sense, I performed a brief Internet search, which revealed several case reports of a patient that sounded identical to this patient —with the same age and history of having an exploratory sternotomy performed to evaluate this complaint. Case reports revealed he had been seen at numerous hospitals across the country from New York to California dating back to at least 2003 [8-13]. I approached the patient with this newfound information with a renewed sense of fair play and invited him to confess to his confabulations. He insisted his pain was real. In collaboration with the on-call cardiothoracic surgeon, we agreed that given his baseline low-likelihood, a CT scan without contrast would be sufficient to rule out significant aortic pathology. This was performed and was, predictably, negative for aortic dissection. It did show a venacaval filter and some small surgical clips in his anterior mediastinum, presumably from his exploratory surgery. I again confronted the patient, this time with a rational sense — with concrete data. At this point he requested to leave and I discharged him.
ADVERTISEMENTSo, what was really going on here?
Malingering
Malingering is characterized by an intentional deception, including both invention and exaggeration, concerning a physical or psychgological condition with the goal of obtaining some external reward, e.g., not having to work, food or shelter, avoiding arrest, etc [14].
One study suggests that the rate of malingering in the emergency department may be as high as 13%, with the belief that in recent years, this has only increased [15,16].
Another study found that among patients with chronic pain, the rate of malingering was between 20 and 50% [17]. By federal law, patients must be screened for an emergency medical condition, so regardless of the so called “red flags,” some sort of an evaluation must be completed. Regardless, malingering must always be a diagnosis of exclusion, and the excluding process costs time and resources.
Munchausen or factitious disorder
Munchausen syndrome, also known as factitious disorder imposed on self (as classified by DSM V), involves more dramatic and convincing presentations by often well-informed patients without an obvious secondary gain. The goal of patients with factitious disorder is often simply to be the center of attention: to be actively cared-for, to play the role of sick patient. They accomplish this by employing deception to exaggerate, fabricate, simulate, or induce their symtpoms [14]. They are often well-informed about their feigned conditions, understandably so as they have typically had numerous diagnostic evaluation and therapeutic interventions for them, and have been so convincing that they often carry scars as a result of these investigations [18].
These patients will often take medications such as insulin or immunosuppressants, or introduce extraneous blood to emesis or urine samples in order to alter laboratory testing and prolong the ruse. They are often confrontational and almost invariably leave against medical advice after health care workers become less compliant to their requests for pain medicine, intervention, or treatment in the face of largely negative evaluations.
Emergency departments are particularly susceptible to these patients as the disorders they mimic often require immediate intervention. An emergency physician must always consider factitious disorder to be a diagnosis of exclusion, so even when one suspects that something is irregular, he or she must nevertheless continue the evaluation and treatment until such devastating diagnoses are excluded. Munchausen by proxy, or factitious disorder imposed on another, involves creation or confabulation of disease in another person, usually a child, with the goal of assuming a central role as the patient’s caregiver.
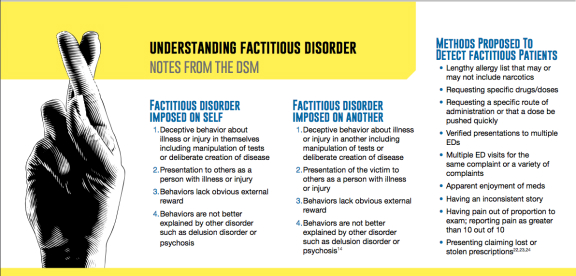
For a listing of diagnostic criteria for factitious disorders, see figure 1:
Somatization or Somatic Symptom Disorder
Somatization disorder is the presence of physical symptoms that, after complete diagnostic evaluation, have not been found to have a physical or organic cause. DSM V has abandoned this diagnosis with the following statement: “It is not appropriate to give an individual a mental disorder diagnosis solely because a medical cause cannot be demonstrated.” They have replaced it with the more specific diagnosis of somatic symptom disorder. Unlike its predecessor, this new diagnosis includes patients whose symptoms can be explained medically as well as those whose cannot.
Patients’ reaction to symptoms is excessive and disproportionate, with high levels of anxiety and excessive energy spent on addressing these symptoms. The most common complaints include pain, gastrointestinal complaints, cardiovascular complaints such as palpitations or shortness of breath, or neurologic complaints such as dizziness, weakness, or paresthesias [19,20]. Somatization disorder has previously been associated with risk factors such as mental illness, sexual abuse, low socio-economic status, minority status, and female sex [19,21].
These patients are often ED recidivists and frequent various specialists who have not been able to give them a diagnosis or present them with a satisfactory treatment plan. The best approach is to have such patients establish care with one primary physician who can track their symptoms over time and monitor for changes that might herald organic disease, while avoiding the problem of multiple providers initiating multiple interventions – which might cause iatrogenic disease. Compliance with this approach has been problematic as this population favors the convenience of emergency departments and often does not make or keep appointments [19].
Factitious disorders, malingering, and somatization or somatic symptom disorder are a problem for the emergency department. These patients are often skilled in deception and well informed about current medical practices and the hesitancy providers may feel to distrust a potentially serious presentation. The [appropriate]concern in medicine – not to miss a serious diagnosis – has allowed patients like the one highlighted above to abuse the healthcare system for years. While few are likely as adept as he, the standard practice of giving the benefit of the doubt allows an impossibly unknown number of others to similarly take advantage of the system in smaller ways.
There have been numerous methods proposed in the past to detect the less veracious patient. These methods are both poorly defined and poorly sensitive.
It should be noted, one study found that several of these behaviors – including lost or stolen prescriptions, pain greater than 10 out of 10, or requesting of a specific route – were present in only a minority of patients who were eventually referred for chemical dependency [24]. Electronic communication systems and databases, including the electronic health record (EHR), are advancements that should improve our ability to detect and avoid redundant management of such patients. These may take many forms including health information exchange between participating hospitals and healthcare facilities (such as the system used to find records about this patient), and state prescription drug monitoring systems. Evidence gleaned from review of such systems can provide a justification to avoid costly and invasive testing.
Various techniques have been employed by ED physicians including direct confrontation and request for identification — as some patients give falsified names or birthdays. These techniques often result in the patient opting to leave the ED without further assessment or treatment. Circulation of aliases and descriptions are problematic due to patient privacy issues, but as many of the more complex perpetrators tend to have well-studied and consistent histories, disseminated information and awareness of these patients without specific data constituting protected health information may be sufficient to raise the level of suspicion for a particular complaint or implausible presentation.
In the psychiatric literature, there are numerous studies designed to define criteria to identify prevaricators. These require complex neurocognitive testing such as the Minnesota Multiphasic Personality Inventory, the Symptom Validity Test, and the Fake Bad Scale that are not reasonable options in the ED, particularly for complaints with potentially devastating outcomes such as dissection [25,26]. One author presents a five-criteria system with a relatively low sensitivity and high specificity that, due to the requirement for neurocognitive testing, is only partially applicable for the ED. His criteria include:
• Presence of external incentive
• Physical findings, defined as perception of poor effort, non-organic cluster of symptoms, discrepancies in story, and changed behavior based upon whether the patient believes he or she is being observed or not
• Compelling inconsistency, e.g. some- one who says he cannot walk and then does
• Lack of other diagnosis that fits the symptoms better [25]
Those who have experience working in an emergency room develop a sense for the gestalt of a drug-seeking patient, an unconscious recognition that may or may not be dependent upon some of the above described criteria. One study comparing the ED provider’s impression to a state prescription drug monitoring program found that such a gestalt had a sensitivity of 63.2% and a specificity of 72.7% for identifying drug-seeking behavior [27]. This suggests that ED physicians likely have a good sense of who is and is not present in the ED for secondary gain. This intuition or awareness of subtle irregularities should cue the practitioner into looking for some of the other more classic characteristics of nefarious intent. This appears to be the most accurate method of detection yet identified barring logistically prohibitive testing.
Those who choose to abuse healthcare resources for their own secondary gain harm not only themselves, but those from whom the resources of time, tests, and therapies are being diverted. To simply acquiesce because it is easier – and it always is – is an impediment to good patient care. Indulging such patients, thinking that our actions have little consequence on the broader picture in the life of either the individual or the healthcare environment at large – adds to the problem. The available studies on rates suggest that EDs are already taxed by demands of increasing patient volume and corporate compliance. Through the use of electronic resources and increasing awareness, we may avoid unnecessary and wasteful care and deliver better service to those who legitimately require it.
1. Leap, Edwin. Second opinion: cynicism well earned, judiciously applied. Emergency Medicine News 2014; 36(3):5.
2. Resnik DB, Rehm M, Minard RB. The undertreatment of pain: scientific, clinical, cultural, and philosophical factors. Med Health Care Philos 2001; 4(3)277-88.
3. Manchikanti L, Helm S, Fellows B, Janata JW, Pampati V, Grider JS, Boswell MV. Opioid epidemic in the United States. Pain Physician 2012; 15(3 Suppl):ES9-38.
4. Nguyen V, Nelson LS, Lenz K, Ung L. Part of the solution? Or part of the problem? Comments on clinician impression versus prescription drug monitoring program criteria in the assessment of drug-seeking behavior in the emergency department. Ann Emerg Med 2014; 63(4):500-1.
5. Hupp JR. Patients using dental pain to obtain narcotics from emergency physicians—a dental perspective. Am J Emerg Med 2014; 32(2014):466-85.
6. Whiteside LK, Walton MA, Bohnert ASB, Blow FC, Bonar EE, Ehrlich P, Cunningham RM. Nonmedical prescription opioid and sedative use among adolescents in the emergency department. Pediatrics 2013; 132(5):825-32.
7. Clouse WD, Hallett JW, Schaff HV, Spittell PC, Rowland CM, Ilstrup DM, Melton LJ. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc 2004; 79(2):176.
8. Gaudina M, Nasso G, Romano V, Pragliola C, Di Cesare A, Speziale G, Massetti M. Acute aortic pathology, Munchausen syndrome, and confirmation bias. J Emerg Med 2013; 45(6):e183-6.
9. Firstenberg MS, Sirak JH, Sun B, Kasick DP. Factitious disorders and cardiothoracic surgery: the ongoing multidisciplinary challenges of a complex case. Case Rep in Med 2009; 2009 ID 103265:1-3.
10. Hopkins RA, Harrington CJ, Poppas A. Munchausen syndrome simulating acute aortic dissection. Ann Thorac Surg 2006; 81:1497-9.
11. Fedoruk LM, Kern JA. Munchausen syndrome and acute aortic dissection: letter 1. Ann Thorac Surg 2006; 82:1948-54.
12. Estrera AL, Safi HJ. Munchausen syndrome and acute aortic dissection: letter 2. Ann Thorac Surg 2006; 82:1948-54.
13. Hopkins RA, Harrington CJ, Poppas A. Munchausen syndrome and acute aortic dissection: reply. Ann Thorac Surg 2006; 82:1948-54.
14. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA. American Psychiatric Association, 2013. 309,311,324-6 p.
15. Yates BD, Nordquist CR, Schultz-Ross RA. Feigned psychiatric symptoms in the emergency room. Psychiatr Serv 1996; 47(9):998-1000.
16. Brady MC, Scher LM, Newman W. “I just saw Big Bird. He was 100 feet tall!” Malingering in the emergency room. Curr Psychiatr 2013; 12(10):33-8,40.
17. Greve KW, Ord JS, Bianchini KJ, Curtis KL. Prevalence of malingering in patients with chronic pain referred for psychologic evaluation in a medico-legal context. Arch Phys Med Rehabil 2009 90:1117-26.
18. Asher R. Munchausen’s syndrome. Lancet 1951; 257(6650):339-41.
19. Stephenson DT, Price JR. Medically unexplained physical symptoms in emergency medicine. Emerg med J 2006; 23:595-600.
20. Kroenke K, Rosmalen JG. Symptoms, syndromes, and the value of psychiatric diagnostics in patients who have functional somatic disorders. Med Clin North Am 2006; 90(4):603.
21. Creed F, Barsky A. A systematic review of the epidemiology of somatisation disorder and hypochondriasis. J Psychosom Res 2004; 56(4):391.
22. McCaffey M, Grimm MA, Pasero C, Ferrell B, Uman GC. On the meaning of “drug seeking.” Pain Manag Nurs 2005; 6(4):122-36.
23. Weiner SG, et al. As the prescribing practices of emergency providers come under enhanced scrutiny, watch for red flags of drug-seeking behavior. ED Manag 2014; 26(1): 5-8.
24. Grover CA, Elder JW, Close RJH, Curry SM. How frequently are “classic” drug-seeking behaviors used by drug-seeking patients in the emergency department? Western J Emerg Med. 2012; 13(5):416-21.
25. Bianchini KJ, Greve KW, Glynn G. On the diagnosis of malingered pain-related disability from cognitive malingering research. Spine J 2005; 5(4):404-17.
26. Berry DTR, Baer RA, Harris MJ. Detection of malingering on the MMPI: a meta- analysis. Clin Psychol Rev 1991; 11(5):585-98.
27. Weiner SG, Griggs CA, Mitchell PM, Langlois BK, Friedman FD, Moore RL, Lin SC, Nelson KP, Feldman JA. Clinician impression versus prescription drug monitoring program criteria in the assessment if drug-seeking behavior in the emergency department. Ann Emerg Med 2013; 62(4):281-9.
while I understand the concern of dealing with patients with this mental condition, I must say that I have been the victim of the other side of the coin. The side where doctors don’t believe me to the point of neglecting to properly read my medical chart. I have several serious health conditions, but I am young and since they are all internal, often don’t show on the outside. I have ulcerative colitis, endometriosis, spodyloarthritis, and recurrent corneal abrasions (the latter two of which are associated with my ulcerative colitis). I am also still recovering from injuries from a car accident I probably should not have lived through. I am allergic to sulfa drugs I do in fact have anaphylaxis in response to these drugs I have anaphylactic reactions to a few things which is why as I write this I have an epi pen and a bottle of Benadryl on my nightstand. When I first was put on sulfa drugs for my ulcerative colitis, I went back in shortly after tell the doctor I think I am allergic to this medicine as my tongue was feeling funny and poofy. The doctor said that the benefits out way the negative and sent me home. Not to long after that I was in the ER surrounded by a frantic team. By the time they had me stable, my face had became so swollen that I had to be on pain meds because my face hurt so bad. I almost died, was in a lot of pain, and stuck in the hospital for 2 days because a doctor didn’t take me seriously. I also have endometriosis, which can often times be confused with the pain of colitis, at least in my case. I may go in there thinking I have one thing, and have the other, and I have been accused of faking my illness. One time a doctor came in while I was the ER for a flare up (which my blood work supported, I waiting for imaging to cone back, and I was in fact having a flare up) and was almost yelling at me saying I was faking my disease, and there is no proof I had it. I was very confused, as I have had a biopsy done, am on medication for it, and have suffered through multiple hospitalizations. Not too long after the supervising physician came in and apologized for that doctor’s behavior and said he knew how horrible my disease was. He was very apologetic, however it was still really horrible of the first doctor to have done what she did. Especially since if she had just looked at my chart she could have seen that I have in fact had a positive biopsy, and that I am in fact on medications for this condition. To be in that much pain and then be accused of being a liar is an awful thing to go through. I think that the doctor who accessed me has no business being a doctor. Being so assumption can risk lives. Recently I went to the ER for a bad flare up. The triage nurse obviously did not take me seriously, as everybody went ahead of me even though I knew that something was quite wrong. I was severely dehydrated, in severe pain, and with severe nausea. I was out in the waiting room for over two hours. I ended up passing out in my chair, at which point I guess they were a worried. They came over to check on me and though I was able to get up, a few steps in I passed out right there in the middle of the ER. They put me on heart monitors and kept me there for quite a few hours to rehydrate me, and keep an eye on my heart. I had an elevated white blood cell count coupled with severe pain in my abdominal area, nausea, and severe dehydration. I was too out of it to be of much use as I was in and out of consciousness and a lot of pain. They hydrated me with some bags of fluid and sent me home with some nausea medicine, They never took an abdominal scan even with the high white blood cell count. They didn’t check my files properly. The next day I was back in except this time in much worse shape, and I had to be hospitalized for several days. All because a doctor didn’t properly check my files. He also acted like I was drug seeking, as I did ask for some pain medication, as I was in extreme pain since my internal organs were swollen! I would like address your red flag list. Lengthy allergy lists that may or may not include narcotics: I do have a lengthy allergy list. Anaphylaxis to sulfa drugs, penicillin shuts down my kidneys (can’t remember the name of the reaction at the moment, but I spent several days in the hospital as a result). I also have a reaction to morphine but not any of the other IV pain meds I have been on. I did not determine this reaction, doctors did one of the times I was hospitalized. I am also very familiar with my allergy and medication list as I have 5 specialists I work with along with my primary care physician. Every time I go to any of those doctors I have to list and review all my allergies and medications. So I basically do this at least 3-4 times a month. Not to mention going to the pharmacy one a month as well. So I suppose it could seem like I memorized something, but it is only because I have to go over it so often. I have also had times where my pain is a 10 out of 10. I have went into shock before from pain before the ambulance got to me. I would say if you’re in so much pain you go into shock then perhaps that qualifies as a 10 out of 10. I frequently have suffered from 8 out of 10 pain. Another red flag you list is being too familiar with your condition. If you gave a chronic and/or life threatening condition, how could you not be very familiar with your condition? I am very familiar with my conditions. It seems it would be irresponsible not to know about your conditions. And after enough hospitalizations and tests, you do start to get the lingo, and have an idea about what is going on. Another red flag you mentioned was asking for specific meds. I have taken enough anti-nausea meds to know that Zofran doesn’t work very well for me, while phenergan does. I also know vicodin makes me throw up within 15 min of taking it. Also, nsaids cause my ulcerative colitis to flare up. This doesn’t mean I am making up my condition.
I totally understand. My allergy list does include some narcotics, so once they hear that they usually start taking me seriously….and give me narcotics anyway because “we have to treat the pain somehow, too.” Ughhh